Have you ever wondered why your doctor switches your prescription from a brand-name drug to a generic version without changing the dose? It’s not just about saving money. It is about science. Specifically, it is about two numbers that determine if two different pills are actually the same inside your body. These numbers are Cmax and AUC. They are the backbone of bioequivalence, the regulatory standard that ensures generic medications work just as well as their expensive brand-name counterparts.
If you are taking medication, understanding these metrics helps you trust the process. You don’t need a degree in pharmacology to grasp the basics, but knowing how peak concentration and total exposure work can clear up a lot of confusion. Let’s break down what Cmax and AUC really mean for your health.
What Is Bioequivalence?
Bioequivalence is the absence of a significant difference in the rate and extent of absorption into the systemic circulation between two drug products. In simpler terms, it means the generic drug gets into your bloodstream at the same speed and in the same amount as the original brand-name drug. If this condition is met, regulators assume the therapeutic effect and safety profile will be identical.
This concept was formalized after the U.S. FDA established its Orange Book system in 1980, building on earlier research from the 1970s. Before this, proving a generic worked required massive clinical trials with hundreds of patients. Today, we use pharmacokinetic studies-measuring blood levels over time-to prove equivalence much faster and cheaper. This shift allows millions of people access to affordable medicine every year.
| Feature | Brand-Name Drug | Generic Drug |
|---|---|---|
| Active Ingredient | Same | Same |
| Dosage Form | Identical (e.g., tablet) | Identical |
| Inactive Ingredients | Specific formulation | May differ slightly |
| Cost | Higher | Lower (typically 80-85% less) |
| Regulatory Requirement | Clinical Trials for Safety/Efficacy | Bioequivalence Study (AUC & Cmax) |
Understanding Cmax: The Peak Concentration
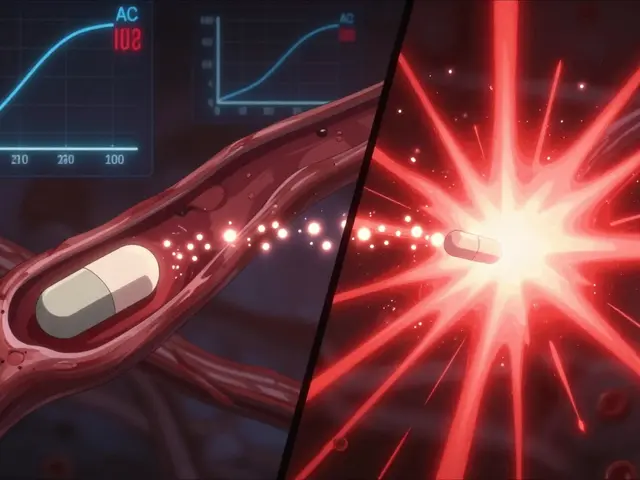
Cmax stands for maximum plasma drug concentration. Imagine drinking a glass of water. Your thirst goes away quickly, but the water stays in your system for hours. Cmax is like the moment the water hits your stomach full force-the highest point of intensity. For drugs, this is the highest level of the medication found in your blood after you take a dose.
Why does this matter? For some drugs, hitting the right peak is crucial for effectiveness. Take painkillers, for example. If the Cmax is too low, the painkiller might not kick in fast enough or strong enough to relieve your headache. On the flip side, if the Cmax is too high, it could cause side effects. This is especially critical for drugs with a narrow therapeutic index, where the line between "effective" and "toxic" is very thin.
Regulators look closely at Cmax to ensure the generic drug doesn’t spike higher than the brand name. If a generic pill dissolves too quickly, it might release all the drug at once, causing a dangerous surge in blood levels. By matching the Cmax, manufacturers ensure the rate of absorption is safe and effective.
Understanding AUC: The Total Exposure
AUC stands for Area Under the Curve. While Cmax tells us about the peak, AUC tells us about the journey. It measures the total amount of drug that enters your bloodstream over time. Think of it as the total volume of water absorbed by your body from that glass, not just how fast it hit your stomach.
AUC is calculated by plotting drug concentration against time and finding the area under that curve. It is expressed in units like mg·h/L. This metric is vital because it reflects the overall exposure your body has to the medication. For most drugs, efficacy correlates directly with total exposure. If the AUC of a generic drug is significantly lower than the brand name, your body simply isn’t getting enough medicine to do its job throughout the day.
For instance, antibiotics need to maintain a certain level in the blood to kill bacteria effectively. If the AUC is too low, the bacteria might survive and develop resistance. Conversely, if the AUC is too high, you risk toxicity. Therefore, matching the AUC ensures that the generic drug provides the same cumulative benefit as the original product.
The 80-125% Rule: How Regulators Decide
You might wonder, "Do they have to be exactly the same?" No. Human bodies vary, and manufacturing processes have slight tolerances. Instead of demanding identical numbers, regulators use a statistical range. The gold standard is the 80%-125% rule.
Here is how it works: Researchers give healthy volunteers both the brand-name and generic versions of a drug in a crossover study. They measure the Cmax and AUC for each. Then, they calculate the ratio of the generic to the brand. For bioequivalence to be approved, the 90% confidence interval of this ratio must fall entirely within 80% and 125%.
This range originated from statistical principles adopted by the FDA and EMA. It assumes that a difference of less than 20% in systemic exposure is not clinically significant for most drugs. Importantly, both Cmax and AUC must independently meet this criterion. If the AUC passes but the Cmax fails, the drug is not considered bioequivalent. This dual requirement protects against issues with both the total dose and the speed of delivery.
Exceptions and Special Cases
Not all drugs follow the standard rules. Some medications are more sensitive than others. Narrow Therapeutic Index (NTI) drugs, such as warfarin (a blood thinner) or levothyroxine (for thyroid conditions), require tighter control. For these drugs, a small change in exposure can lead to serious health consequences.
Regulatory agencies like the EMA recommend tighter limits for NTI drugs, often narrowing the acceptance range to 90%-111%. This means the generic must be almost identical to the brand in terms of exposure. Additionally, highly variable drugs-where individual patients react differently-may use scaled average bioequivalence methods. This approach adjusts the limits based on the variability of the reference product, ensuring fair assessment without compromising safety.
How Bioequivalence Studies Are Conducted
These studies are rigorous and tightly controlled. Typically, they involve 24 to 36 healthy volunteers. Participants receive one version of the drug, wash out (wait until the drug leaves their system), and then receive the other version. Blood samples are taken at multiple time points-often 12 to 18 times-over several days.
Modern labs use LC-MS/MS technology, which can detect drug levels as low as 0.1 ng/mL. This precision allows scientists to map the exact concentration-time profile. The data is then analyzed using specialized software like Phoenix WinNonlin. Statistical analysis involves logarithmic transformation of the data, as pharmacokinetic parameters follow a log-normal distribution. This step is crucial for accurate comparison.
One common pitfall is inadequate sampling during the absorption phase. If blood isn’t drawn frequently enough in the first few hours, Cmax might be underestimated. Regulatory guidances emphasize using actual sampling times rather than nominal ones to avoid errors. Despite these challenges, over 90% of bioequivalence studies today yield reliable results, supporting the approval of thousands of generic drugs annually.
Is Cmax more important than AUC?
Neither is universally more important; they serve different purposes. AUC ensures the total dose is adequate for efficacy, while Cmax ensures the rate of absorption is safe and effective. Both must pass regulatory criteria for bioequivalence approval. For drugs where peak levels cause side effects, Cmax is particularly critical. For drugs requiring sustained presence, AUC is key.
Why is the bioequivalence range 80-125% and not 90-110%?
The 80-125% range is symmetrical on a logarithmic scale, which matches the natural distribution of pharmacokinetic data. It allows for a reasonable margin of error (up to 20% difference) that is generally not clinically significant for most drugs. Tighter ranges like 90-110% are reserved for narrow therapeutic index drugs where small differences matter more.
Can I switch between generics of the same drug?
Generally, yes. Since all approved generics meet the same bioequivalence standards relative to the brand name, they should perform similarly. However, if you notice changes in effectiveness or side effects when switching manufacturers, consult your doctor. Individual sensitivity to inactive ingredients can sometimes vary.
What happens if a generic fails bioequivalence testing?
If a generic fails to meet the 80-125% criteria for either AUC or Cmax, it cannot be approved for sale. The manufacturer must reformulate the drug-perhaps changing the excipients or manufacturing process-and conduct new studies. This rigorous process ensures only equivalent products reach the market.
Do bioequivalence studies test for long-term safety?
No, bioequivalence studies are short-term (usually a few weeks) and focus on pharmacokinetics in healthy volunteers. Long-term safety and efficacy were already established during the initial clinical trials of the brand-name drug. The assumption is that if the exposure (AUC) and peak (Cmax) are equivalent, the long-term outcomes will also be equivalent.