

If you or a loved one has myasthenia gravis, picking the right drug can feel like a maze. Mestinon is often the first name that pops up, but several other pills work just as well for different needs.
Mestinon is the brand name for pyridostigmine bromide, an oral acetylcholinesterase inhibitor that boosts muscle strength by slowing the breakdown of acetylcholine. It’s taken by most patients shortly after diagnosis because it’s easy to dose and has a relatively gentle side‑effect profile. However, cost, dosing frequency, and personal tolerance can push people to look at alternatives.
Key Takeaways
- Mestinon (pyridostigmine) remains the first‑line oral treatment for most myasthenia gravis patients.
- Neostigmine offers a fast onset but requires frequent dosing and close monitoring.
- Amifampridine (3,4‑diaminopyridine) is useful for patients with severe fatigue or those who can’t tolerate pyridostigmine.
- Choosing the right medication depends on onset speed, dosing convenience, side‑effects, and insurance coverage.
- Always discuss any switch with a neurologist experienced in neuromuscular disorders.
How Mestinon Works and Who It Helps
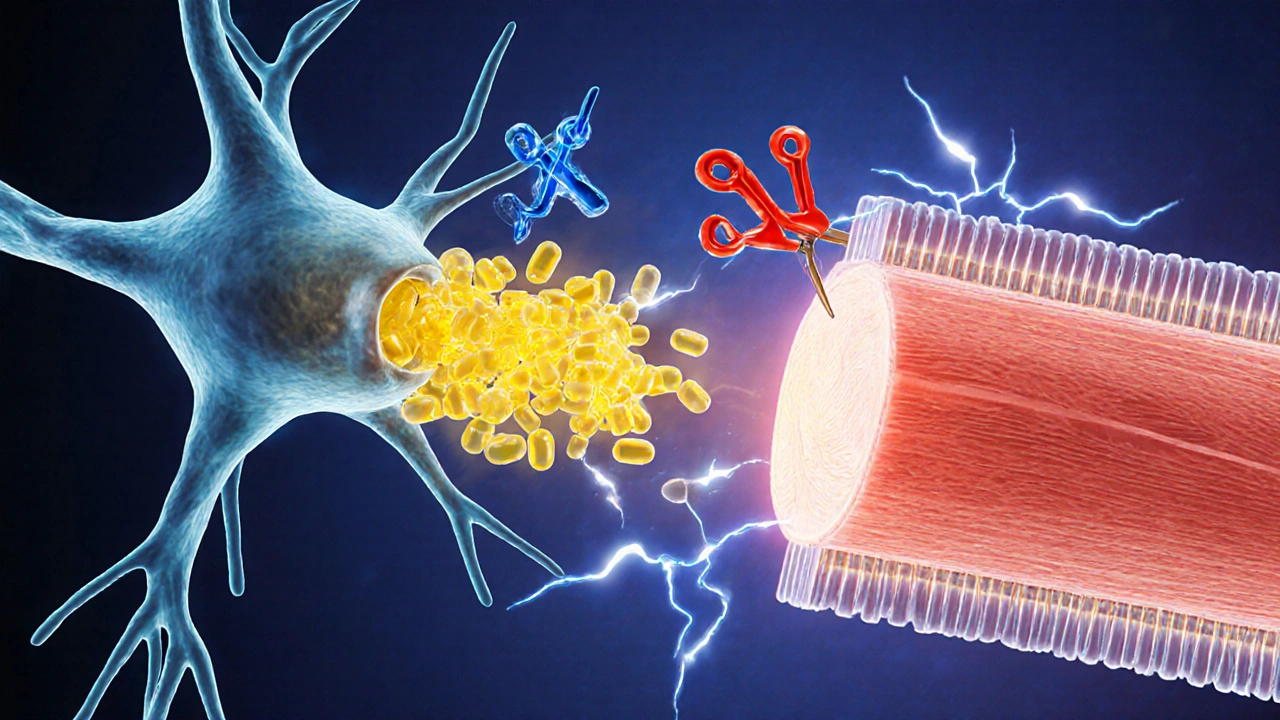
Pyridostigmine is a reversible acetylcholinesterase inhibitor that temporarily blocks the enzyme that breaks down acetylcholine at the neuromuscular junction. By keeping more acetylcholine available, muscles receive stronger signals, reducing the characteristic weakness of myasthenia gravis.
Typical adult dosing starts at 60mg three times daily, titrated up to 60mg every 4-6hours as needed. Most patients notice improved eye‑muscle control and less overall fatigue within a week.
Alternative AChE Inhibitors: Neostigmine
Neostigmine is another reversible acetylcholinesterase inhibitor, traditionally given by injection for short‑term muscle control during surgery or in acute MG crises.
Its onset is rapid-within minutes-but the effect lasts only 2-4hours, so patients often need 4-6 doses per day. Because it can cause more gastrointestinal cramping, it’s usually reserved for patients who need quick symptom relief or cannot tolerate oral pills.
Amifampridine (3,4‑Diaminopyridine): A Different Mechanism
Amifampridine works by blocking potassium channels, which prolongs the action potential in nerve endings, allowing more acetylcholine to be released.
It’s taken twice daily, and many users report steadier energy throughout the day. FDA approval for Lambert‑Eaton myasthenic syndrome (LEMS) opened the door for off‑label use in MG, especially for patients who still have fatigue despite optimal pyridostigmine dosing.
When Immunosuppressants Join the Mix
Sometimes AChE inhibitors aren’t enough. Doctors may add immunosuppressants such as Azathioprine or Mycophenolate mofetil. These drugs don’t act on acetylcholine directly; they calm the immune system so fewer antibodies attack the receptors.
While not a direct alternative to Mestinon, they are part of the broader treatment landscape. Patients often stay on a low dose of pyridostigmine while the immunosuppressant reaches full effect (several months).
Comparison Table: Mestinon and Its Main Alternatives
| Brand / Generic | Onset | Duration | Typical Dose | Common Side Effects | Approx US Cost (30‑day supply) |
|---|---|---|---|---|---|
| Mestinon (pyridostigmine) | 30-60minutes | 4-6hours | 60mg 3-6×daily | Diarrhea, abdominal cramps, increased saliva | $30-$70 (generic) |
| Neostigmine | 5-10minutes (injectable) | 2-4hours | 0.5-2mg 4-6×daily (oral) or 1-2mg IV/IM as needed | Muscle cramps, nausea, sweating | $15-$40 |
| Amifampridine | 1-2hours | 6-12hours | 10-20mg twice daily | Tremor, headache, urinary urgency | $1,200-$1,800 (specialty drug) |
| Azathioprine | Weeks (immune effect) | Long‑term | 50-150mg daily | Liver enzyme elevation, nausea, increased infection risk | $30-$60 |
Decision Checklist: Which Drug Fits Your Life?
- Need quick relief? Choose neostigmine for rapid onset, but be ready for more frequent dosing.
- Prefer once‑ or twice‑daily dosing? Amifampridine’s longer half‑life may suit busy schedules.
- Budget matters? Generic pyridostigmine (Mestinon) is the most affordable option.
- Sensitive stomach? Some patients tolerate neostigmine better than pyridostigmine, while others find amifampridine’s side‑effects milder.
- Long‑term disease control? Combine low‑dose pyridostigmine with an immunosuppressant instead of switching drugs.

Potential Pitfalls and How to Avoid Them
Switching from Mestinon to another AChE inhibitor can trigger a temporary flare‑up if the new drug’s onset is slower. To smooth the transition, doctors often overlap doses for 24-48hours while monitoring muscle strength.
Another common mistake is stopping pyridostigmine abruptly, which can cause a myasthenic crisis-rapid worsening of breathing muscles. Always taper under medical supervision.
Real‑World Stories
Emily, a 32‑year‑old teacher, started on 60mg Mestinon three times a day. She loved the flexibility, but a new job required early mornings. Her neurologist switched her to amifampridine 20mg twice daily. Within two weeks Emily reported steadier energy and fewer bathroom breaks during class.
James, 58, experienced severe abdominal cramps on pyridostigmine. After a trial of low‑dose neostigmine, his cramps vanished, though he now takes the drug every four hours. He balances the schedule with a mobile reminder app.
When to Come Back to Your Doctor
Schedule a follow‑up if you notice any of these: difficulty swallowing, worsening eyelid droop, new shortness of breath, or side‑effects that interfere with daily life. Blood tests may be needed when adding immunosuppressants.
Frequently Asked Questions
Can I take Mestinon and neostigmine together?
Only under strict medical supervision. Combining two AChE inhibitors can cause excessive acetylcholine, leading to muscle twitches, excessive salivation, and potentially dangerous heart rhythm changes.
Is amifampridine covered by insurance?
Coverage varies. Some private insurers treat it as a specialty drug and require prior authorization. Medicare Part D may cover it with a high copay. Check with your pharmacy benefits manager for exact details.
What should I do if I miss a dose of Mestinon?
Take the missed dose as soon as you remember, unless it’s almost time for the next scheduled dose. In that case, skip the missed pill and continue with your regular schedule. Never double‑dose.
Are there natural ways to boost acetylcholine?
Choline‑rich foods like eggs, liver, and soy can support acetylcholine synthesis, but they don’t replace prescription AChE inhibitors. Always discuss supplements with your neurologist.
How long does it take for azathioprine to work?
Azathioprine usually shows clinical improvement after 2-3months, with full effect sometimes taking up to a year. That’s why many patients stay on a low dose of pyridostigmine during the waiting period.





Comments (14)
Kevin Galligan
October 6, 2025 AT 15:45 PMAlright folks, if you’ve ever felt like your meds are a riddle wrapped in an enigma, you’re not alone 😊. Mestinon is the “starter pack” for MG, cheap and easy, but don’t expect it to solve every problem. Think of it like the reliable friend who shows up to every party-comforting, yet sometimes a bit predictable. If you need a switch, just remember you’re the boss of your own dosage schedule, and your doc’s there to back you up.
Dileep Jha
October 14, 2025 AT 00:20 AMWhile the prevailing narrative glorifies pyridostigmine as the de‑facto first‑line, one must interrogate the pharmacokinetic ceiling imposed by its cholinergic saturation. The ontogeny of synaptic transmission in MG patients reveals a non‑linear dose‑response curve, rendering neostigmine’s rapid onset a superior modulatory vector in certain phenotypes. Moreover, the ion channel blockade mechanism of amifampridine circumvents the acetylcholinesterase bottleneck altogether, offering a paradigm shift in therapeutic hierarchy.
Michael Dennis
October 21, 2025 AT 08:54 AMIt is evident that the article provides a comprehensive overview of the available agents. However, the discussion lacks depth regarding long‑term safety profiles, particularly for immunosuppressants. The comparative table, though informative, would benefit from inclusion of patient‑reported outcome measures. Overall, the piece serves as a reasonable introductory guide.
Blair Robertshaw
October 28, 2025 AT 16:29 PMHonestly this post is a bit of a mess, they left out the real side effects of neostigmine like the crazy cramps that can ruin your day. Also they make it sound like amifampridine is cheap, which is total bs – it’ll cost you a small fortune. They could’ve at least mentioned that some ppl just can’t handle pyridostigmine at all.
Alec Maley
November 5, 2025 AT 01:04 AMI totally understand how overwhelming the drug choices can feel, especially when your energy levels are already low. Remember that each medication has its own rhythm, and finding the right match often involves a bit of trial and error with your neurologist. Keep tracking your symptoms, and don’t hesitate to voice any concerns about side‑effects – your comfort matters.
Navjot Ghotra
November 12, 2025 AT 09:39 AMSwitching meds is okay if you monitor closely
Claus Rossler
November 19, 2025 AT 18:14 PMIt would be a folly to accept the conventional hierarchy without scrutinizing the ethical dimensions of pharmaceutical economics. The commodification of amifampridine, priced exorbitantly, betrays a market that prioritizes profit over patient autonomy. Yet, one must also acknowledge that such pricing reflects the research investments underlying its novel mechanism.
chris mattox
November 27, 2025 AT 02:49 AMHey friends, let’s think of these meds as different colors on a palette – each brings a unique hue to the canvas of your daily life. Mestinon might be the steady blue, neostigmine a vibrant orange for quick bursts, and amifampridine a calming green that lasts longer. Blend them wisely with your doc’s guidance, and you’ll paint a clearer picture of strength.
Jackson Whicker
December 4, 2025 AT 11:23 AMWhen we contemplate the labyrinthine corridors of myasthenia gravis therapy, we are not merely choosing a pill; we are engaging in an existential dialogue with our own mortality. The humble Mestinon, with its modest cost and familiar dosing schedule, stands as the faithful sentinel at the gate of symptom control, yet it is also the emblem of therapeutic inertia that tempts complacency. In contrast, neostigmine bursts onto the scene like a mercurial troubadour, offering rapid relief that can be both a boon and a curse, demanding the patient’s relentless attention to timing and side‑effects. Amifampridine, the newcomer with its potassium‑channel blockade, promises a more sustained vigor, but it does so at a price that can feel like a hereditary tax imposed on the vulnerable. One must weigh not only the pharmacodynamics but also the sociocultural weight of insurance formularies that dictate access, turning a clinical decision into a bureaucratic battlefield. The immunosuppressants, Azathioprine and Mycophenolate, linger in the background, whispering of long‑term horizons while the patient battles the present. Yet, the specter of a myasthenic crisis looms whenever a medication is altered without careful overlap, a reminder that the neuromuscular junction is a fragile alliance. Consider the patient narrative: a young professional juggling early mornings may find the twice‑daily rhythm of amifampridine liberating, whereas an elderly retiree might prefer the familiarity of daily Mestinon. The side‑effect profiles are not mere footnotes; gastrointestinal cramps can rupture daily plans, while tremors from amifampridine can erode confidence. Ultimately, the art of medicine resides in the dialectic between evidence and individual experience, a dance choreographed by the neurologist and the patient alike. Thus, when you stand before the table of options, ask not which drug is superior in abstract, but which one aligns with your life’s cadence, your financial reality, and your tolerance for risk. The answer is rarely singular; it is a mosaic composed of dosage, timing, support, and unwavering communication. In the end, the best drug is the one that empowers you to rise each morning a little steadier than the last, and that is the true victory over myasthenia gravis. Remember that regular follow‑up appointments serve as checkpoints on this therapeutic odyssey, allowing adjustments before crises emerge. Empower yourself with a symptom diary, noting strength fluctuations and adverse events, for this data becomes the compass guiding future tweaks.
Audrin De Waal
December 11, 2025 AT 19:58 PMLook, we all know the West pushes pricey drugs like amifampridine while our own local generics hold the line. It’s a reminder that true health sovereignty comes from trusting the tried‑and‑true Mestinon, not bowing to foreign pharma giants.
parag mandle
December 19, 2025 AT 04:33 AMAllow me to elucidate: when transitioning from pyridostigmine to any alternative, the key lies in a calculated overlap period of 24–48 hours, during which plasma concentrations are meticulously monitored. This strategy mitigates the risk of a transient dip in acetylcholine availability, which could otherwise precipitate a perilous myasthenic crisis.
Shivali Dixit Saxena
December 26, 2025 AT 13:08 PMWhen choosing a medication, consider onset, duration, side‑effects, cost, and personal lifestyle,; this holistic view ensures optimal adherence,; and enhances overall quality of life.
Sayam Masood
January 2, 2026 AT 21:43 PMIn the grand tapestry of therapeutic choices, each drug represents a thread woven with intention; to discern the pattern, one must balance empirical evidence with the patient’s lived narrative, thereby crafting a personalized symphony of care.
Jason Montgomery
January 10, 2026 AT 06:18 AMHey everyone, keep sharing what’s working for you and stay patient with the trial‑and‑error process – you’ve got this, and the right fit will come along.